FeaturesMEMBER EXCLUSIVE

Japan has introduced an innovative strategy to combat antibiotic resistance. Should the United States adopt a similar approach?(Image credit: Nicoletta Lanese (left and right panels); Getty Images (central panel); edited by Live Science)
- Facebook
- X
- Reddit
- Pinterest
- Flipboard
Share this article 0Join the conversationFollow usAdd us as a preferred source on GoogleSubscribe to our newsletter’A Silent Pandemic’: How Japan Is Curbing Antibiotic Resistance, One $5 Incentive at a Time
Antimicrobial resistance is a grave public health threat, often termed a “silent pandemic,” yet it receives scant attention. To mitigate resistance, healthcare providers must prescribe antibiotics judiciously and with utmost responsibility. This analysis is the inaugural piece in a series examining antibiotic consumption patterns in Japan and the United States, with a specific emphasis on pediatric outpatient care. This work was facilitated by a reporting grant from the Association of Health Care Journalists and The Commonwealth Fund.
Approximately ten years ago, the Japanese government identified a concerning trend: pediatricians were widely dispensing antibiotics, far exceeding the requirements for treating diagnosed bacterial infections.
Antibiotics are effective against bacterial infections but not those caused by viruses, fungi, or parasites. Nevertheless, medical practitioners frequently provided young patients with antibiotics for ailments unlikely to be bacterial in origin. Administering antibiotics for non-bacterial infections can foster antimicrobial resistance (AMR) and contribute to the proliferation of superbugs by unnecessarily exposing bacteria to these drugs, thereby compelling them to develop survival mechanisms. These resistant bacteria can then transmit their acquired resistance traits to others, exacerbating the issue.
In the long term, resistance could render common infections untreatable with current medications, escalating the risk of severe illness and mortality across the population.
When Japanese pediatricians did treat bacterial infections, they often opted for antibiotics that contribute to resistance — specifically “broad-spectrum” agents that act against a wide range of bacteria. In a 2015 comparative study involving 35 high-income nations, Japan ranked last in the appropriateness of antibiotic selection for children under five years of age.
One method to decelerate the emergence of AMR is to enhance control over antibiotic prescriptions. Consequently, Japan concentrated its efforts on one of its most significant sources of problematic antibiotic use: pediatric outpatient facilities.
“These clinics present a particular challenge,” stated Dr. Yusuke Okubo, chief of clinical epidemiology and health services research at the National Center for Child Health and Development, a research institution and hospital located in Tokyo. Examining Japan’s overall antibiotic consumption, “90% of prescriptions originate from outpatient clinics, not hospitals,” Okubo informed me. (Outpatient practices account for a comparable percentage of antibiotic prescriptions in the U.S.)
A substantial portion of inappropriate prescriptions were issued to children younger than three years old, particularly those presenting with upper respiratory tract infections, which are viral in origin approximately nine out of ten times, according to Okubo. Gastroenteritis, or stomach flu, was another prevalent condition for which antibiotics were frequently overprescribed, despite most cases being viral.
Government officials conceived an idea: What if each instance a pediatrician opted against prescribing an antibiotic in these circumstances resulted in a modest financial incentive — a reward for making a more prudent choice? Each incentive would be small, currently equating to about $5 based on today’s exchange rate, but could cumulatively amount to thousands of dollars in annual income for individual clinics. This represents a significant sum for Japanese pediatricians, whose annual earnings Okubo estimates to be between $90,000 and $100,000.
This incentive scheme, implemented in 2018, has proven successful, leading to its expansion to encompass a broader range of patients, clinics, and conditions. But what contributed to the program’s effectiveness? I traveled to Japan to investigate the systemic and cultural factors that underpinned its success, with the ultimate goal of determining if other nations, such as the U.S., could draw valuable lessons from this nationwide initiative.

Historically, Japanese pediatricians frequently prescribed antibiotics, but an insurance-based system is now facilitating a change in this practice.
(Image credit: Susumu Yoshioka via Getty Images)The Stealthy Rise of Resistance
In the realm of bacteria, as in nature, survival favors the fittest. Exposure to antibiotics results in the demise of a proportion of bacteria, while others endure. This surviving population possesses characteristics that enable them to resist the drug’s effects, encoded within “resistance genes.” Bacteria can transmit these genes to subsequent generations through reproduction and can also directly transfer them to neighboring bacteria. Furthermore, they are capable of acquiring new resistance genes via random DNA mutations.
All antibiotics carry the inherent risk of exerting pressure on bacteria to develop resistance; this is a fundamental property of these medications. However, broad-spectrum agents pose the greatest hazard, as they impact a wider array of bacteria compared to narrow-spectrum drugs. The 2015 cross-national comparison revealed that Japanese physicians prescribed antibiotics with the lowest resistance risk only 35% of the time, indicating that the majority of antibiotic prescriptions were for broader-spectrum agents.
While the use of broad-spectrum drugs is sometimes necessary, such as when an infection is refractory to narrow-spectrum options, their application when not warranted accelerates the development of AMR. The same applies to the use of antibiotics for non-bacterial infections. In both scenarios, evolutionary pressure is introduced that could have otherwise been averted.

Evidence indicated that pediatricians in Japan frequently prescribed antibiotics for common childhood illnesses that were likely caused by viruses. Overprescription was a particularly significant issue for children under the age of three.
(Image credit: recep-bg via Getty Images)
Globally, resistance is escalating among prevalent bacterial pathogens, far outpacing the development of alternative treatments to antibiotics. In 2021, infections caused by resistant bacteria directly resulted in 1.14 million fatalities worldwide and were a contributing factor in an additional 3.57 million deaths. These figures are projected to increase substantially by 2050 if decisive action is not implemented promptly.
Common pathogens already exhibit high levels of resistance in Japan, and resistant germs are responsible for thousands of deaths annually, primarily affecting older adults. Individuals aged 65 and above constitute approximately 30% of Japan’s population. As this demographic continues to grow in the coming years, health officials anticipate a potential rise in AMR-related illnesses.
Japan’s youngest inhabitants are also susceptible, as resistant bacteria can occasionally be transmitted from mothers to newborns during birth, leading to severe complications like sepsis. Resistance has also been observed in respiratory pathogens that commonly affect children, such as Mycoplasma pneumoniae, according to Dr. Takemi Murai, deputy head of the Infectious Diseases Division at Nagano Children’s Hospital in Azumino. “There have been outbreaks of Mycoplasma that are resistant to antibiotics,” he noted.
However, not long ago, the unrestricted administration of antibiotics was a standard practice in Japanese medical care. (The numerous reasons for this will be explored in subsequent installments of this series.)
National insurance data, sampled from 2005, indicated that 60% of patients in Japan with non-bacterial upper respiratory tract infections received antibiotic prescriptions, predominantly broad-spectrum types like third-generation cephalosporins, macrolides, and quinolones. The majority of these prescriptions originated from clinics.
A change was imperative.
Recommendations for Appropriate Treatment
In 2016, Japan intensified its commitment to reducing antibiotic misuse by releasing its inaugural National Action Plan on Antimicrobial Resistance. This initiative aligned with a global strategy set forth by the World Health Organization, aiming to enhance awareness of AMR and optimize the utilization of antimicrobials, including antibiotics, among its member states.
Two significant objectives for Japan were to reduce overall antibiotic consumption by 33% and broad-spectrum antibiotic usage by 50% by the year 2020. The nation narrowly missed achieving these ambitious targets by the stipulated deadline, a feat that was no small accomplishment. The incentive program was merely one component of a comprehensive set of measures introduced to improve AMR awareness and antibiotic prescribing practices.
The Japanese government produced posters to raise public awareness regarding AMR. This particular example features the well-known anime character Amuro Ray, whose given name shares phonetic similarities with “AMR,” creating a pun that enhances the campaign’s appeal.
(Image credit: Courtesy of Dr. Yusuke Okubo)
Prior to the incentive’s inception, Japan’s Ministry of Health, Labour and Welfare (MHLW) — whose responsibilities are comparable to those of the U.S. Department of Health and Human Services — initiated educational campaigns targeting both healthcare providers and patients. They also published a manual on antibiotic usage, with the initial edition primarily directed at outpatient physicians. This manual emphasized that most acute respiratory tract infections and acute diarrheal diseases do not necessitate antibiotic treatment.
Among children, those under five years of age exhibited the highest rates of antibiotic prescriptions, frequently receiving these medications for respiratory infections. Data indicated that this overprescription issue was most pronounced in children under three years old being evaluated for upper respiratory infections or acute gastroenteritis. The government’s proposed remedy? To provide additional remuneration to physicians for withholding antibiotics in cases where they were not medically indicated.
“If the clinicians provide more appropriate medical services, we add additional payment,” stated Dr. Takuma Kato, a counselor at the Permanent Mission of Japan to the United Nations, who formerly worked on the incentive program for MHLW. In such instances, they offer “a little bit more” compensation when physicians refrain from prescribing antibiotics for illnesses presumed to be viral, he explained.
“A little bit more” is an accurate description. Each incentive payment amounts to 800 yen, which was approximately $7.20 at the program’s launch in April 2018 and is about $5 based on current exchange rates.
Here’s how the system operates: A guardian brings their infant or toddler experiencing illness for an initial consultation, and the pediatrician diagnoses a likely acute upper respiratory tract infection or gastroenteritis. Given that these conditions are typically viral, the physician decides against prescribing an antibiotic. The doctor communicates this reasoning to the guardian and offers guidance for home care. If the appointment meets these criteria, the clinic is eligible to receive an additional 800 yen when submitting their reimbursement claim.
Since mild viral infections generally resolve on their own within a few days, a strategy known as “watchful waiting” can help determine if a bacterial infection is indeed the underlying cause. Therefore, if a physician prescribes an antibiotic during the initial visit, they often advise the guardian to return with the child if their condition remains unchanged or deteriorates within a few days. The incentive and this “waiting” approach are complementary strategies.
Certain technical conditions apply. For instance, the children being evaluated must not have any pre-existing conditions that could complicate their case, such as a compromised immune system. If children test positive for influenza or COVID-19 through a formal diagnostic test, the incentive is not applicable. To qualify for the incentive, clinics must specialize in pediatrics and operate under a “comprehensive” payment structure, meaning patients pay a standardized fee for the entire visit rather than an itemized “fee-for-service” model prevalent in the U.S.
Despite these specific stipulations, the incentive offers a valuable benefit to the clinics that utilize it. “I believe pediatric doctor associations are very pleased,” Okubo commented.
Physicians Assert “Small Incentives Accumulate”
The Japanese government generally employs strategies that incentivize physicians to modify their practices, rather than imposing penalties for suboptimal conduct, according to Okubo.
“It conveys a constructive message from the government: ‘You have altered your behavior, so we will provide compensation,'” Okubo explained. “This positive approach motivates physicians, particularly pediatricians, to apply their sound judgment in their clinical practice.”
This system is readily accepted by Japanese doctors, who have historically wielded considerable political influence, Kato pointed out. Much like in the U.S., their professional organizations, such as the Japan Medical Association, engage in lobbying efforts with the government and typically oppose policy proposals perceived as detrimental to their financial interests.
Conversely, an incentive-based approach is “very, very welcome, especially by the doctors’ associations,” stated Dr. Norio Ohmagari, director of disease control and prevention at the National Center for Global Health and Medicine, which is part of the Japan Institute for Health Security (JIHS) in Tokyo. Ohmagari also heads the AMR Clinical Reference Center, collaborating with the WHO on AMR countermeasures.
Dr. Yusuke Shibata has been providing medical care at the Shibata Pediatric Clinic in Tokyo since the 1990s. He finds the incentive beneficial, as it not only increases his income but also aligns with his belief that the indiscriminate use of antibiotics should be avoided.
(Image credit: Nicoletta Lanese)
The physicians I interviewed confirmed their positive reception of the incentive, primarily attributing it to the enhancement of their financial returns.
“I submit a claim for the pediatric antibiotic appropriate use support premium every time” it is applicable, said Dr. Yusuke Shibata, proprietor of the Shibata Pediatric Clinic in Asakusa, a historic area within Tokyo’s Taito ward. “I value the premium, as pediatric clinics generally operate with lower profit margins” compared to facilities serving adult patients, Shibata communicated via email following my visit to his clinic.
For initial consultations with children under six years of age, clinics receive a base payment ranging from 6,040 to 7,210 yen, which translates to approximately $38 to $45 at current exchange rates. An additional 800 yen (roughly $5) represents an increase of over 10% to this fee — “a substantial amount,” Okubo emphasized.
Shibata estimates that his clinic treats approximately 30 to 40 patients weekly with acute respiratory infections or diarrhea, depending on the season. He has the potential to claim the incentive for the initial visit of each of these patients, provided they meet the eligibility criteria and do not have disqualifying conditions.
At the higher end of estimates, Shibata projects that he might claim the incentive up to 180 times during a particularly busy month, resulting in a total of 144,000 yen, or approximately $900.
Dr. Atsushi Miyahara, affiliated with the Karugamo Clinic in Tokyo, frequently utilizes the antibiotic incentive. He has long advocated for careful antibiotic usage, and the incentive serves as a reward for his diligent practices.
(Image credit: Nicoletta Lanese)
Dr. Atsushi Miyahara, who manages the Karugamo Clinic in the Setagaya-ku ward of Tokyo, mentioned that he was already conservative in his antibiotic prescribing habits, and thus the incentive offers recognition for his consistent approach.
When Miyahara established his clinic fifteen years prior, he observed that many other physicians prescribed a high volume of antibiotics, leading him to question the practice due to its potential to foster resistance. He distributes informational pamphlets to his patients, detailing the risks associated with resistance and explaining how avoiding unnecessary prescriptions can mitigate this risk. When antibiotics are deemed necessary, he primarily selects narrow-spectrum agents that present a relatively low risk of promoting resistance.
Miyahara stated that the local government and medical associations announced the antibiotic incentive upon its launch, and he perceives its introduction as having been highly beneficial. It has enhanced his revenue and reinforced his commitment to maintaining his stewardship practices. He estimates that for every fifty initial patient visits he conducts, he claims the incentive approximately ten to fifteen times, indicating its applicability to at least 20% of those consultations.
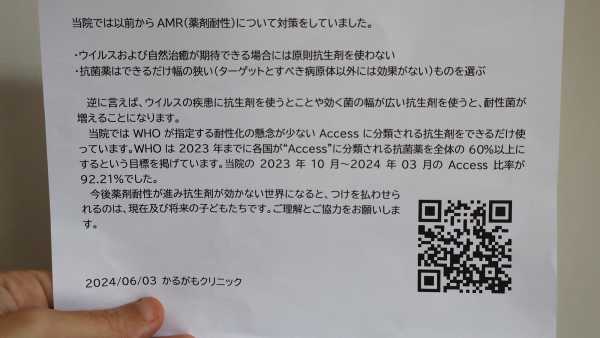
Dr. Atsushi Miyahara provides his patients with an informational flyer that outlines the clinic’s measures against AMR, explaining that antibiotics are not used for viral illnesses and that for bacterial infections, the narrowest-spectrum options are prioritized.
(Image credit: Nicoletta Lanese)The Incentive’s Influence
Given that certain pediatric clinics were eligible for the incentive while others were not — due to the exclusion of fee-for-service clinics — Okubo and his colleagues were able to directly quantify the policy’s efficacy.
To evaluate the incentive’s impact during its first year, researchers analyzed insurance claims from over 10,000 medical facilities from periods immediately preceding and following the policy’s implementation. Approximately 3,000 of these facilities were eligible and submitted claims for the incentive 316,770 times, totaling 253 million yen ($2.29 million at the time). These eligible clinics experienced a 17.8% reduction in their overall antibiotic consumption over the year, with no adverse patient outcomes, such as increased hospitalization rates, observed.
Science Spotlight

(Image credit: Marilyn Perkins / Future)
Science Spotlight provides an in-depth examination of emerging scientific advancements, offering readers essential insights into these developments. Our articles highlight trends across various scientific domains, illustrate how new research challenges established theories, and demonstrate how scientific progress is transforming our understanding of the world.
To ascertain the persistence of these effects, the research team analyzed several years of data from over 165,000 young children who received care at either eligible or ineligible clinics. Within the initial month of the policy’s implementation, the former group of children showed a reduction in total antibiotic prescriptions by nearly 45%, in contrast to the latter group. Cumulatively over the subsequent four years, their overall antibiotic usage and broad-spectrum antibiotic usage decreased by 20% and 24%, respectively.
The decline in antibiotic prescriptions was not accompanied by an increase in hospitalizations or healthcare expenditures, although there was a marginal rise in the total number of physician visits. Okubo explained that this outcome is anticipated, as physicians monitor infections over time, suggesting they employed the watchful-waiting strategy and advised parents to seek follow-up care if improvement was not rapid.
Okubo’s research team has continued to monitor antibiotic prescribing patterns among pediatricians and has observed “spillover effects” in age groups not covered by the incentive. Among individuals under twenty years old, outpatient antibiotic prescriptions decreased by 50% between 2011 and 2022. He posits that the incentive program is a primary driver of this trend, directly reducing prescriptions for the youngest children while also generating ripple effects in older demographics. (This research is slated for upcoming publication in a peer-reviewed journal.)
Nevertheless, there remains scope for enhancing the selection of antibiotics when they are prescribed, as the ratio of broad-spectrum to narrow-spectrum drugs continues to be excessively high. “While total antibiotic use has been reduced, its quality requires further improvement,” Okubo remarked.

Okubo conducts research at the National Center for Child Health and Development in Tokyo. This institution, which is Japan’s largest children’s hospital and a research center, is dedicated to advancing the understanding of child health and development while providing cutting-edge medical care.
(Image credit: Nicoletta Lanese)The Incentive’s Evolution
Although the 800-yen incentive has proven substantial for clinicians, it represents a very small portion of the government’s overall healthcare expenditure, which amounted to 468 billion yen ($3.1 billion) in 2022.
“This program is modest in scale compared to the entire budget,” Dr. Kosuke Sasaki, a member of MHLW’s health insurance bureau, informed me. The program’s budget does not have a fixed upper limit; consequently, if the number of claims from clinics increases, there is no ceiling on the total payout. “The number of physicians utilizing this program has risen while the number of antibiotic prescriptions has declined since its inception,” added Dr. Tomonori Aoki, Sasaki’s colleague, noting that the government anticipates and accommodates the associated costs.
The program’s demonstrable impact and economical cost likely contribute to its expansion over the years.
Every two years, Japan’s Ministry of Finance allocates a portion of the national budget to MHLW, which then revises the pricing for pharmaceuticals, medical devices, and healthcare services. The antibiotic incentive is subject to this revision process and has been enhanced multiple times.

The Ministry of Health, Labour and Welfare is housed in a modest building in Central Tokyo. It is responsible for establishing the national prices for pharmaceuticals, medical devices, and healthcare services.
(Image credit: Nicoletta Lanese)
During its initial revision in 2020, the incentive was extended to cover children under the age of six. In 2022, ear, nose, and throat (ENT) specialists became newly eligible for the incentive; similar to pediatricians, they treat numerous acute infections in children and are prone to overprescribing antibiotics, according to insurance data. In the same year, physicians could begin claiming the fee for treating ear infections and sinus infections.
“I observe a trend where pediatric clinics tend to avoid prescribing antibiotics, but I do notice some ENT clinics prescribing them carelessly,” Shibata, the clinic owner in Asakusa, Tokyo, informed me. This suggests that ENT specialists are a logical group to target next.
In 2024, a separate incentive, administered at the facility level, was introduced as a supplementary measure to the 800-yen incentive. This new program encourages clinics to submit data to a government repository that monitors antibiotic usage. If first-line, narrow-spectrum antibiotics constitute a certain proportion of a clinic’s total prescriptions, that clinic receives additional remuneration, Okubo explained.
Related stories
- Dangerous ‘superbugs’ are a growing threat, and antibiotics can’t stop their rise. What can?
- Antibiotic found hiding in plain sight could treat dangerous infections, early study finds
- Metal compounds identified as potential new antibiotics, thanks to robots doing ‘click chemistry’
Ultimately, the 800-yen incentive has successfully brought AMR to the forefront of awareness for physicians who may not have previously considered it a critical issue, unlike experts such as Kato, for whom “AMR is kind of my life’s work.” Kato and researchers like Okubo regard the program as successful, although they acknowledge areas where antibiotic selection could be further optimized. Ministry officials like Sasaki and Aoki describe the program as straightforward to implement and impactful. Clinic physicians such as Shibata and Miyahara appreciate the incentive and consistently utilize it. In summary, at just $5 per claim, the incentive has proven remarkably effective.
Through discussions with experts in both Japan and the U.S., I have learned that physicians in the United States have historically encountered similar pressures and exhibited comparable lapses in antibiotic use to those observed in Japanese doctors. However, the U.S. does not currently possess an incentive program analogous to Japan’s. The question arises: Should such a program be implemented?
In the subsequent installment of this series, I will delve into a pivotal aspect of this issue: the underlying motivations for pediatricians’ misuse of antibiotics. What are these motivations, and do they differ between physicians in the U.S. and Japan? Understanding these factors will be crucial in determining whether a comparable incentive could yield similar results in both countries.
TOPICS