
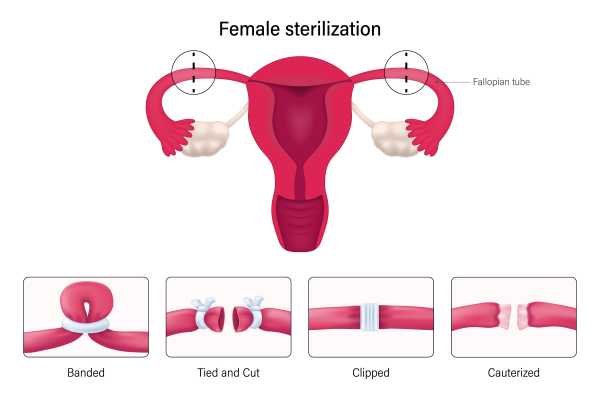
In gynecological practice, there are four key approaches to blocking the fallopian tubes: radical excision of both organs or their closure by coagulation, clips or snares. Some of these techniques are shown in the illustration above. (Image: BSIP/Getty Images)
The term “tubal ligation” is commonly used to refer to surgical sterilization, which involves blocking the fallopian tubes to prevent conception.
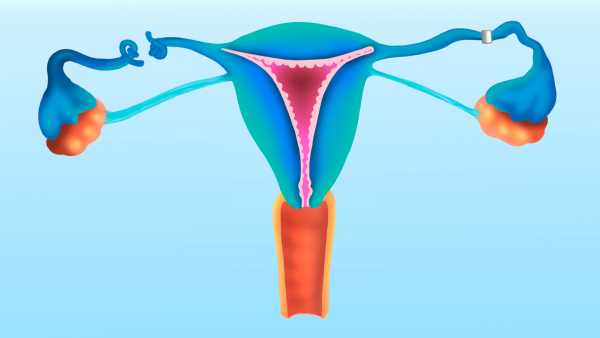
In natural conditions, when a woman conceives, the female reproductive cell migrates from the ovary to the uterine cavity through the fallopian tubes. Blocking these pathways by ligation, clipping, or removal prevents the egg from moving and making contact with the sperm. Salpingectomy—removal of the tubes—is one form of this procedure.
The effectiveness of the method reaches 99% in preventing pregnancy. In operations with extensive access to the pelvic organs (in contrast to minimally invasive techniques), the reliability approaches 100%.
You might be interested
-

How does emergency contraception work?
-

Male Contraception: First Successful Safety Tests of Pills
-
Unique video: the process of embryo implantation in real time
“It's an effective method of contraception, but it does require surgery,” said Dr. Andrew Rubenstein, chief of obstetrics and gynecology at NYU Langone Health.
According to the Cleveland Clinic, possible side effects include shoulder discomfort, bloating, abdominal cramping, nausea, and dizziness. The shoulder pain is due to the gas that temporarily expands the abdominal cavity during surgery and can linger in the tissue for several days.
Rubenstein emphasized that previous pregnancies are not a contraindication to the procedure.
Regardless of the timing of the operation, a detailed discussion between the patient and the doctor, sometimes involving the partner, is a mandatory step.
“The decision is made collectively,” Rubenstein noted, “this is not a one-time consultation, but a process that requires a trusting dialogue.”
How is the procedure performed?
The four main techniques for blocking the fallopian tubes include complete removal (bilateral salpingectomy, or “bisalp”) or isolation through coagulation, clipping, or snare ligation.
(Removal of one tube, unilateral salpingectomy, does not result in sterilization, but is used for pathologies such as ectopic pregnancy.)
The choice of approach depends on the patient's medical history: age, surgical history, BMI and other factors influence the technique, Rubenstein noted.
The operation is usually performed through tiny incisions: below the navel and in the lower abdomen.
Laparoscopic instruments, including a miniature camera and manipulators, allow the surgeon to visualize and perform procedures.
Sometimes the procedure is performed to prevent ovarian cancer, as studies indicate a link between tumors and the fallopian tubes.
“The risk is not eliminated completely, but it is significantly reduced,” Rubenstein comments. Some studies have found a 24-42% reduction in the likelihood of cancer.
Experts in the field of gynecological oncology recommend considering salpingectomy as a preventive measure for women who are not planning pregnancy and are preparing for pelvic surgeries.
Rubenstein emphasized that some medical institutions refuse the procedure for religious reasons, requiring patients to go to secular clinics.
Is this reversible?
Although rare, there are cases of fertility restoration after surgery – so-called “sterilization failures”.
“Such situations are exceptional,” Rubenstein noted, “but are more often observed in young patients.” In the first year after the intervention, the failure rate does not exceed 0.1–0.8%.
Some doctors avoid operating on patients under 30 because of the risk of regret. A 2022 study found that 12.6% of those under 30 and 6.7% of those over 30 had regrets. The majority of respondents were over 30.
The overall regret rate is comparable to that seen with joint replacement (around 10%).
Rubenstein emphasized: “Many people mistakenly perceive the procedure as a reversible blocking, similar to tying shoelaces.”
RELATED MATERIALS
— Complete twisting of the fallopian tube caused the girl’s emergency hospitalization
—First real-time ovulation video
—An unusual case: the birth of a child after 29 weeks of development outside the womb
Technically, restoration of tubal patency is possible with partial preservation (coagulation, clips), but most doctors recommend IVF. After recanalization, pregnancy occurs in 73% of patients, and childbirth occurs in 53% of patients.
“The effectiveness of IVF in such cases is extremely high,” Rubenstein noted. “We recommend transferring embryos into the uterus, bypassing the tubes.”
Disclaimer
The material is for informational purposes only and does not replace medical advice.

Perry Thaler Social Link Navigation Intern
Perry Thaler is a Live Science intern with interests in space exploration, technology, and natural sciences, as well as environmental and climate issues. Education: astronomy and economics (Cornell University), NASA experience, paleomagnetism research at Harvard. Currently pursuing a master's degree in journalism at NYU, published at ScienceLine, Space.com, and Eos.
Sourse: www.livescience.com



