in InterviewMEMBER EXCLUSIVE

The U.S. had eliminated measles, but now, the country is seeing a resurgence that may signal that the disease has reestablished itself.(Image credit: Shutterstock)Share this article 0Join the conversationFollow usAdd us as a preferred source on GoogleSubscribe to our newsletter
Decades ago, the United States successfully eradicated measles by implementing measures to halt the virus’s consistent transmission within its borders — but it is now probable that measles has returned.
As 2025 drew to a close, health professionals warned that the U.S. might lose its “measles elimination status” within months due to numerous ongoing outbreaks nationwide. Should the U.S. officially forfeit this status, signifying sustained measles transmission for over a year, it would join nations like the U.K. and Canada, which have also experienced localized measles resurgence linked to declining vaccination rates.
An evaluation of the United States’ elimination status is slated for November. In the interim, experts have released a national progress report. Live Science consulted with two contributors to the report from Boston Children’s Hospital — Dr. Anne Bischops, a pediatrician and postdoctoral research fellow, and Maimuna Majumder, a distinguished scholar in the Computational Health Informatics Program — to ascertain the current standing of America’s elimination status and anticipate future developments.
Nicoletta Lanese: Measles cases began to increase in the U.S. around January 2025. Were you concerned at that point about the country losing its elimination status?
Maimuna Majumder: I have personally been engaged with measles research for over a decade, and considering that history, I must say my apprehensions regarding elimination status considerably predate January 2025.
When January 2025 arrived, I felt it might represent a point of no return. However, it was by no means the initial warning sign. I wish to emphasize that achieving and maintaining measles elimination has always been a precarious endeavor, inherently so. Sustaining this elimination status is, by its nature, a challenging feat.
When you observe these localized clusters escalating into outbreaks that threaten to spread to adjacent states, and when you witness the speed at which minor outbreaks develop into larger ones — those tend to be the indicators that signal, “I don’t believe we’ll be able to contain this situation anymore.”
Dr. Anne Bischops: The trend of rising vaccine-preventable diseases has been evident for several years, impacting daily life even in emergency rooms. We’ve encountered an increasing number of measles cases. Particularly following the COVID-19 pandemic, we’ve observed a surge in vaccine fatigue contributing to this trend.
This has become a progressively significant global concern. Regarding the current outbreak in the U.S., our research team has been closely monitoring it since its inception.
NL: What distinct factors characterize our present situation compared to previous measles outbreaks?
MM: My very first engagement with a domestic measles response was during the Disneyland measles outbreak in late 2014 and 2015. That was a different era. The political administration was radically different; culturally, it was a vastly different period regarding the United States’ stance on vaccines. It presented an optimal window for implementing policies that would help safeguard our elimination status.

A significant measles outbreak occurred at Disneyland just over a decade ago.
(Image credit: FREDERIC J. BROWN via Getty Images)
In response to the Disneyland outbreak, we saw the passage of SB-277 in California and various other crucial vaccination bills across the United States, which facilitated the elimination of personal belief exemptions, for instance. This led to remarkable progress in restoring our collective protection against measles.
Over the subsequent decade, substantial changes have occurred. We are now in the second Trump administration, and an intervening massive pandemic has significantly eroded public trust in public health and vaccines. This erosion is largely fueled by the pervasive spread of misinformation.
When the Disneyland outbreak occurred, there was a prevailing sense of optimism that we could leverage the situation to enact protective legislation for Americans. However, the onset of the [2025] Texas outbreak resulted in the opposite scenario. This is when the probability of losing our status becomes imminent, as the mechanisms typically employed to regain elimination status are no longer effective.
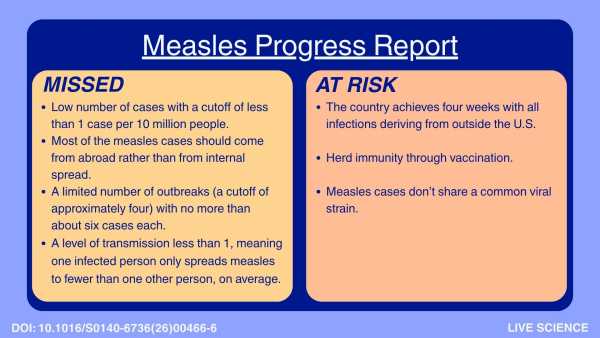
NL: In your report, you outline seven indicators required for a country to achieve elimination status, noting that the U.S. has now failed to meet — or essentially, missed — four out of the seven. Why is it beneficial to define these indicators?
AB: The Pan American Health Organization [PAHO] conducts recertification meetings [such as the one scheduled for November] where highly detailed, granular data for every transmission chain are presented, a process that is very time-consuming.
We observed that the meeting was rescheduled from April to November, prompting our objective with the seven indicators: to establish an early warning framework preceding that decision, utilizing readily accessible data. We have focused on the broad national level, employing only national estimates. We view this as a rapid assessment preceding the November meeting, where an in-depth analysis of transmission chains will be conducted, meticulously tracing each one.
(Image credit: Live Science)
NL: For the indicators that have not yet been “missed,” do we suspect they have been missed but the data is simply not yet available to confirm?
AB: Precisely. For instance, concerning the genotyping criteria, we possess some samples that already indicate a shared genotype. However, we lack the comprehensive genotyping data for every single transmission chain. Therefore, we surmise this criterion may have been missed, but confirmation requires a detailed analysis.
Regarding vaccine coverage, we only have estimates for kindergartners [concerning the proportion of kindergarteners who are up-to-date on measles vaccination], and we do not have immunity data. Nonetheless, based on the available information, we can infer that this criterion has likely already been missed.
NL: Experts have suggested that we are likely underreporting our current measles cases. Is this assessment accurate?
MM: I personally concur that an undercount is highly probable. One contributing factor is that measles, in general, may not exhibit severe pathology. Consequently, some children may become ill, and their parents might not seek medical attention. Considering the methodology for infectious disease surveillance in the U.S., for mandatory reportable diseases like measles to be recorded, an interaction with the healthcare system is necessary. If a disease occurs where this may not always happen, then naturally, an undercount of the disease is to be expected.
Our most reliable indicator is wastewater surveillance [where pathogens are detected in wastewater], yet currently, we do not conduct extensive wastewater surveillance for measles. The subsequent question is how we can improve our tracking methods, which presents a potential avenue for enhancement.
NL: Do you believe wastewater surveillance could be feasibly expanded? I understand that current coverage varies significantly by state.
MM: The technology is available, making this endeavor possible. What poses a challenge — and this applies to all wastewater surveillance, not exclusively for measles — is that our interpretation of wastewater signals remains, to put it frankly, quite rudimentary.
We observe an increase in viral presence in wastewater, indicating a rise in community infections. The accuracy of this scaling factor is contingent upon numerous variables, making a precise 1:1 correlation between wastewater data and the actual number of cases in a community at any given time exceedingly difficult.
A significant factor, naturally, is the vulnerability of wastewater data to rainfall [as rainfall dilutes wastewater, necessitating adjustments for accurate interpretation]. Consequently, numerous physical engineering considerations are involved that we have not yet fully resolved. It is challenging to state definitively, “There are precisely this many cases because there is this much wastewater indication of this disease in this location.” We are not yet capable of making such precise determinations in a meaningful way.
What we can accomplish is utilizing wastewater data to anticipate increases in respiratory disease hospitalizations and predict when upticks in primary care provider visits for a particular illness might occur — wastewater surveillance is highly effective for these predictive purposes. I believe there is substantial room for improvement in this area, and it is an achievable goal.
Massachusetts is a leading state in wastewater surveillance, boasting its own dedicated surveillance teams. Therefore, if I were to identify states likely to pioneer a measles wastewater program, Massachusetts would be among the most probable candidates.
NL: Your report suggests we are on the verge of losing our elimination status, with increased vaccination rates identified as a primary solution. Will this effort predominantly occur at the state and local levels, given the federal government’s position?
MM: All our states function as autonomous entities responsible for their respective health management, meaning we lack a multitude of universally applied national programs. Even in the absence of Trump’s presidency, we would anticipate most vaccination campaigns to be executed at a more localized level; this has consistently been the practice.
However, we now face a federal government that is quite firmly opposed to vaccines, even as figures like RFK Jr. are retracting earlier statements and asserting, “Actually, vaccines are acceptable.” There is considerable indecisiveness even at the federal government level, which warrants acknowledgment. I would characterize this not as vaccine hesitancy at the federal level, but rather as skepticism. This skepticism sows doubt, which then has a cascading effect on individuals residing in various states.

Measles vaccines are highly effective in preventing measles infections and the subsequent severe outcomes and long-term complications.
(Image credit: FatCamera/Getty Images)
The public discourse surrounding vaccines is significantly shaped by federal pronouncements.
While federal discourse does not impede states’ legislative authority to enact measures protecting their populations through enhanced vaccination, it undeniably influences public perception of vaccines within those states. The majority of individuals in this country are more attuned to federal politics than to state-level affairs; this reflects the current reality.
This leads to a situation where, despite the federal government possessing limited authority over state mandates for school entry, it exerts influence through its communication strategies, reaching individuals nationwide.
AB: From a pediatrician’s viewpoint, we can observe numerous vaccine-promoting campaigns daily, yet a single brief online comment can propagate widespread doubt. Therefore, as a pediatrician, I find it crucial to exercise extreme caution in health communication. I believe concerted efforts are necessary at all levels.
NL: Is there any other key takeaway you hope people gain from your progress report?
MM: Given the global resurgence of measles and the number of other countries that have similarly lost their status or are nearing that point, we believe this [framework] could also be beneficial for other nations as an early warning mechanism.
This issue is not unique to the U.S.; it is not occurring in isolation.
The political landscape in most high-income countries exhibits comparable trends that are undeniably influencing the prevalence of this issue. The fact that numerous high-income countries have lost their measles elimination status in the past year strongly indicates this. However, it is important to note that politics is not the sole factor; systemic memory also plays a role.
By systemic memory, I refer to the current generation of parents who have never personally known someone severely affected by measles. They have no awareness that in previous generations, this disease caused fatalities or left individuals with debilitating long-term health conditions. This lack of direct experience can lead to a perception that the disease is not particularly serious.
When public health initiatives are successful, their effectiveness often goes unnoticed — a common observation within our field. The reason measles did not pose a threat during my childhood was the widespread vaccination coverage. This situation is challenging; it is inherently human to question the severity of something when one has not personally witnessed its consequences.
NL: To date, all indications suggest the U.S. will lose its status in November. Do you concur?
MM: I would be quite surprised if the outcome were different. While I would be delighted if a turnaround were possible, it appears unlikely.
This outcome might be averted if our society collectively decides that the stringent criteria previously applied are no longer desirable. We could potentially retain elimination status by altering the criteria, effectively moving the goalposts. If such a change occurs, I would find it deeply unsatisfactory.
Either we lose the status because the criteria remain unchanged and no progress is made, which appears to be the most probable scenario, or we retain status due to a revision of the criteria, driven by a reluctance to be perceived as failing. The least likely, yet most positive, possibility is that we collectively manage to address the situation effectively within the next six months without altering the criteria.
AB: There are no standardized criteria or definitive cutoffs for determining elimination status. Ultimately, the decision rests entirely with the expert panel convened in November, so the precise benchmarks they will employ remain unknown. However, based on the data currently available, it is highly probable that we will, regrettably, lose our status.
NL: Could the expert panel adjust the benchmarks, as you mentioned?
AB: The Centers for Disease Control and Prevention [CDC] has established an expert panel responsible for conducting the analysis and subsequently presenting their findings to the Pan American Health Organization meeting in November.
MM: That is precisely why I suggested the second option is a possibility. Panel members possess the authority to determine that the criteria differ.
Related stories
- Measles has long-term health consequences for children. Vaccines can prevent all of them.
- ‘I don’t know if the CDC will survive, to be quite frank’: Former CDC officials describe the agency’s disintegration under RFK
- The U.S. is on track to lose its measles elimination status in months. RFK needs to be removed. [Opinion]
NL: However, if PAHO deems the presented data invalid, could they state that?
MM: They have the capacity to do so — whether they will is a separate matter. The World Health Organization [WHO] and its affiliated bodies [such as PAHO] typically do not hesitate to issue statements when they believe certain governments are not being truthful. This tends to occur in highly politicized situations where the data originating from a country is perceived as unreliable.
The WHO has indeed made such pronouncements in the past. However, the U.S. represents a distinct entity. I believe we are now confronting the question of whether it would excessively harm the WHO and PAHO to take a stance against the CDC. This is a complex question without a clear-cut answer at present.
To address your question directly, can they do it? Yes, they can. There is precedent for other countries. But the U.S. is not just any nation, and we must acknowledge that.
As a region, we have already relinquished that status [given that Canada has already lost its elimination status]. My hope is that this would foster greater honesty among all parties. I do feel that the situation would be significantly more tense if the U.S. were the deciding factor in whether the Americas retained their elimination status.
Editor’s note: This interview has undergone minor edits for conciseness and clarity. Live Science conducted the interview with Bischops and Majumder in May, so the content may not reflect subsequent developments.